
Every week at Health & Style Medical Centre, we see patients who arrive with a variation of
the same story. They went to their doctor because of back pain — pain that had been
getting in the way of their daily life for months, sometimes years. They had an X-ray or an
MRI. The doctor looked at the scan, then looked at the patient, and said something along
the lines of: “There is some degeneration here, but that is normal for your age. You will just
have to manage it.”
And the patient went home believing that their pain was inevitable, irreversible, and
something they would simply have to live with.
This is one of the most common and most harmful misconceptions in musculoskeletal
medicine.
Spondylosis is real. Spinal degeneration is real. But the equation of degeneration with
permanent, untreatable pain is not — and accepting it without seeking appropriate
physiotherapy treatment is costing thousands of Abu Dhabi residents their quality of life
unnecessarily.
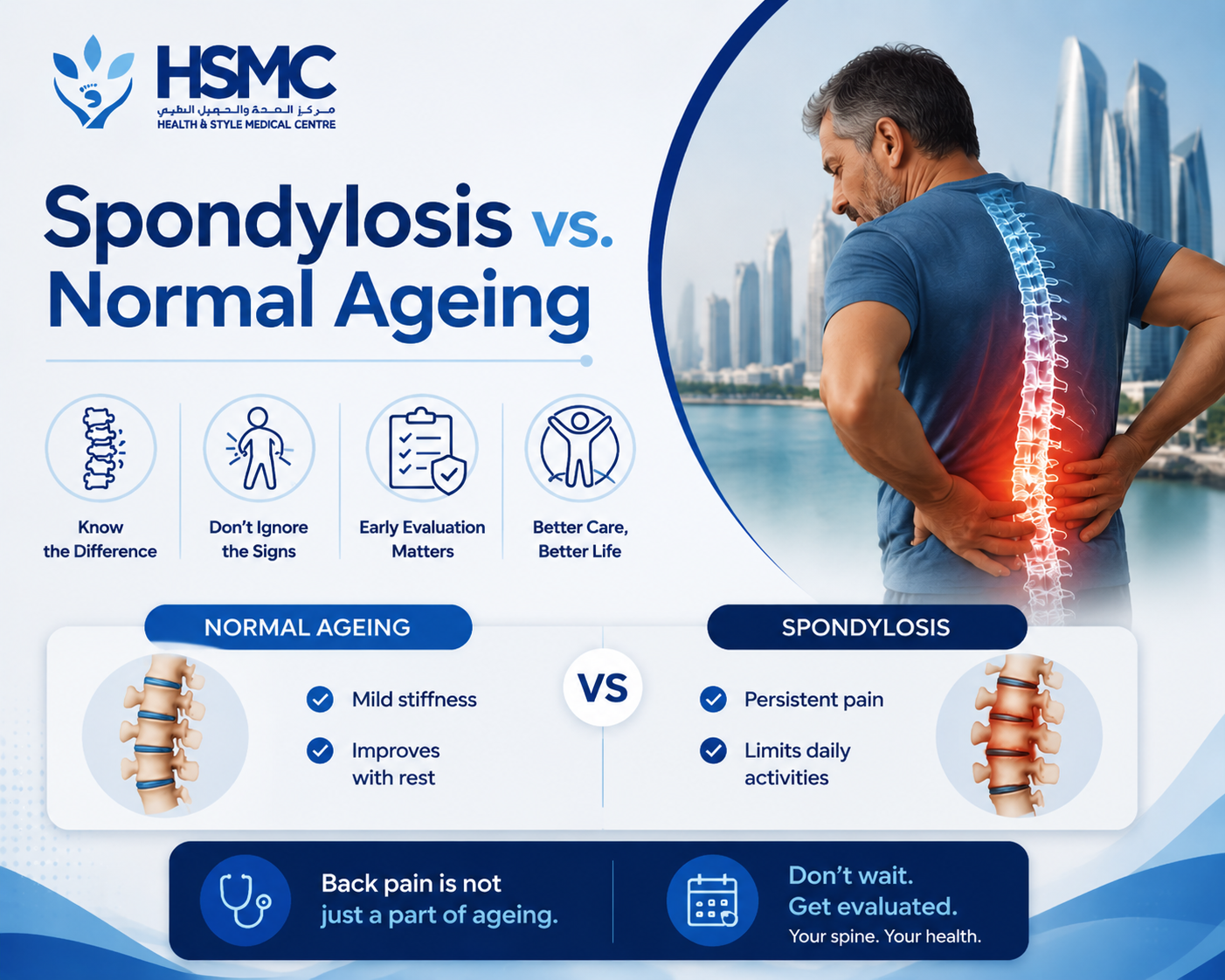
This article will explain what spondylosis actually is, how it differs from normal ageing, why
imaging findings are so frequently misinterpreted, and what physiotherapy can genuinely
achieve for patients with degenerative spinal changes
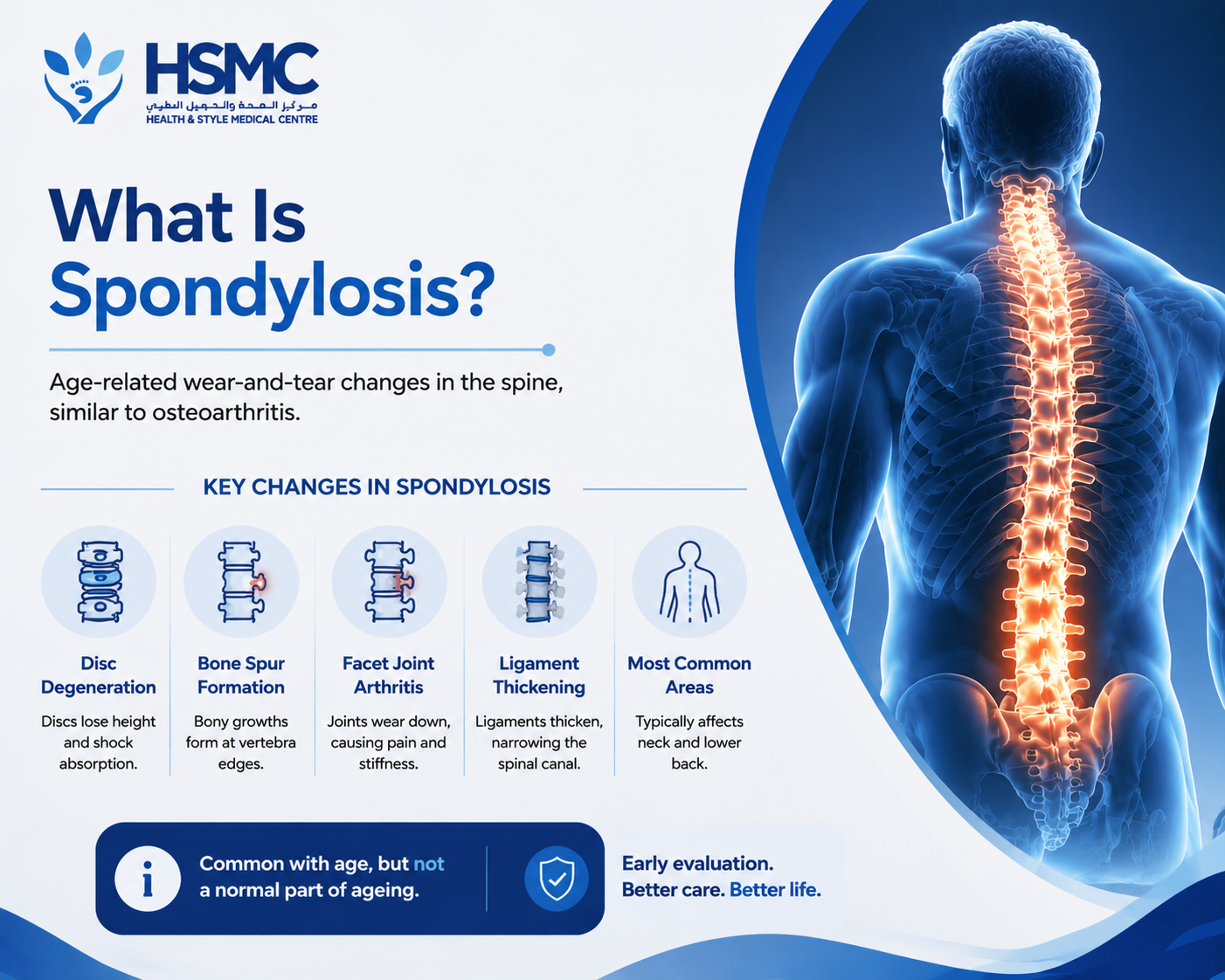
What Is Spondylosis?
Spondylosis is a broad term that refers to age-related, degenerative changes in the spine. It
is essentially the spinal equivalent of osteoarthritis — a gradual wear-and-tear process that
affects the intervertebral discs, the facet joints, and the vertebral bodies themselves
The changes associated with spondylosis include:
Disc degeneration. As the discs age, they lose water content and height, becoming thinner
and less able to absorb shock effectively. The outer fibres of the disc may develop small
tears, and the disc may bulge outward as its structural integrity is reduced.
Osteophyte formation. The body responds to disc degeneration by attempting to stabilise
the affected spinal segment — often by forming bony outgrowths called osteophytes at the
edges of the vertebral bodies. These can be seen clearly on X-ray and are often described
as “bone spurs.”
Facet joint arthritis. The facet joints — the small joints at the back of each vertebra — can
develop arthritic changes similar to those seen in peripheral joints like the knees and hips,
with cartilage loss, joint space narrowing, and inflammatory changes.
Ligament thickening. The ligaments within the spinal canal can thicken over time,
potentially contributing to narrowing of the space available for the spinal cord and nerve
roots — a condition known as spinal stenosis.
Spondylosis can occur at any level of the spine but is most commonly seen in the cervical
(neck) and lumbar (lower back) regions, which are the most mobile — and therefore most
loaded — segments
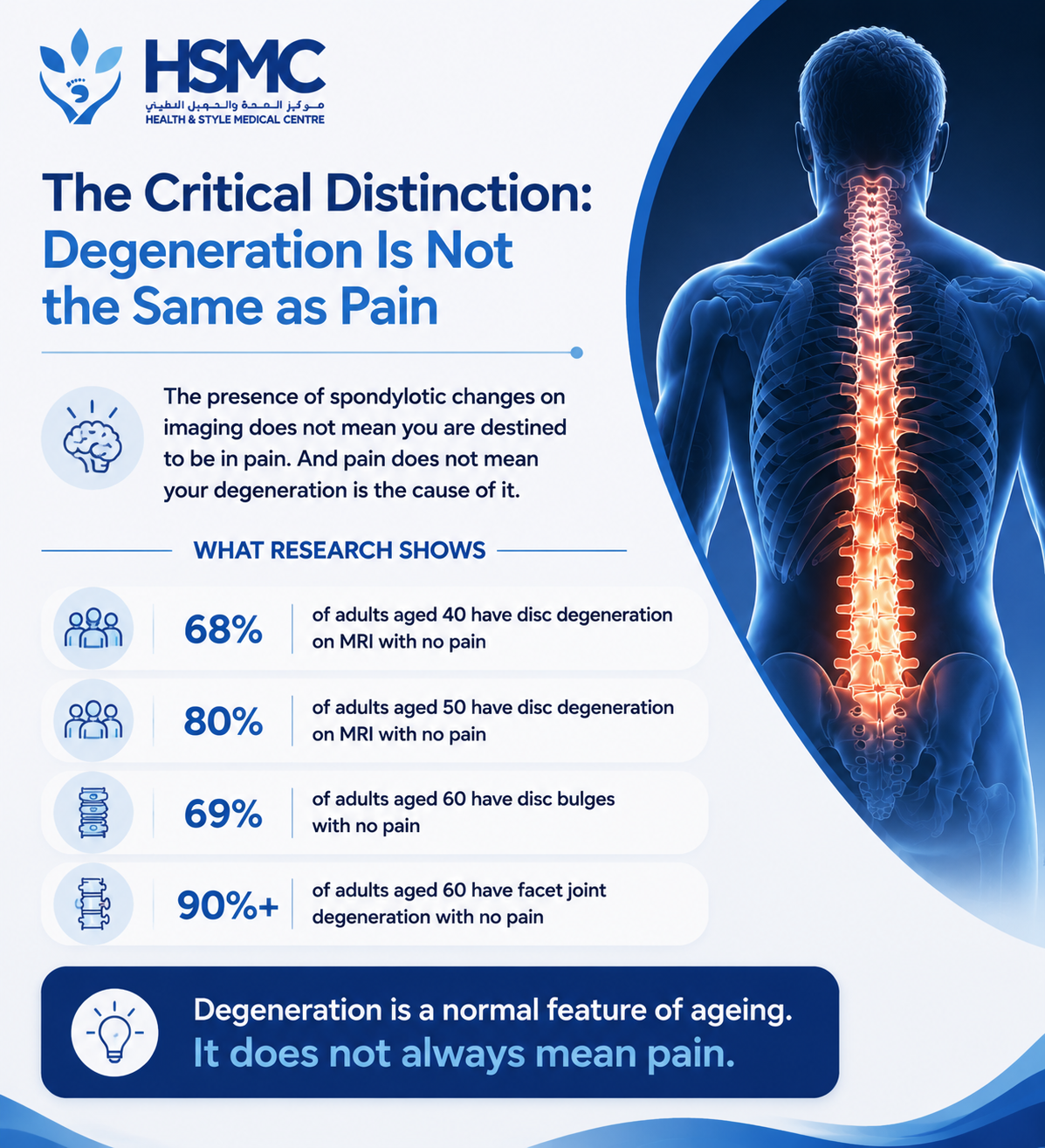
The Critical Distinction: Degeneration Is Not the Same as Pain
Here is the most important thing this article can tell you: the presence of spondylotic
changes on imaging does not mean you are destined to be in pain. And the presence of pain
does not mean your degeneration is the cause of it.
This is not a reassuring platitude. It is a well-established scientific finding
Multiple large-scale studies have used MRI to examine the spines of people with no back
pain whatsoever — no symptoms, no history of significant spinal problems. The findings are
striking:
- In adults aged 40, disc degeneration is visible on MRI in approximately 68% of individuals with no pain
- In adults aged 50, this rises to around 80%
- In adults aged 60, disc bulges are present in approximately 69% of asymptomatic individuals
- Facet joint degeneration is visible in over 90% of adults aged 60 regardless of pain status
In other words, the vast majority of adults over 50 have spinal degeneration visible on
imaging — and most of them have no significant pain.
This tells us something profound: degeneration is a normal feature of the ageing spine, not
a direct cause of pain. The relationship between what is visible on a scan and what a patient
experiences is far more complex than “degeneration equals pain.”
Why Doctors Sometimes Get This Wrong
The misattribution of pain to degenerative changes on imaging is understandable. When a
patient in pain has a scan that shows degeneration, it is natural to connect the two. But this
connection is frequently incorrect — and the consequences of making it can be significant.
Patients who are told their pain is caused by wear and tear that is “normal for their age”
often:
- Stop seeking active treatment, believing nothing can help
- Reduce their activity levels, which weakens the muscles that support the spine and makes pain worse
- Develop a fear of movement, believing that activity will cause further damage
- Experience increased psychological distress, which amplifies pain perception
- Miss the actual, treatable cause of their pain — which may have nothing to do with the degeneration visible on their scan
The problem is not the diagnosis of spondylosis itself. The problem is what is often implied
by it — that nothing can be done.
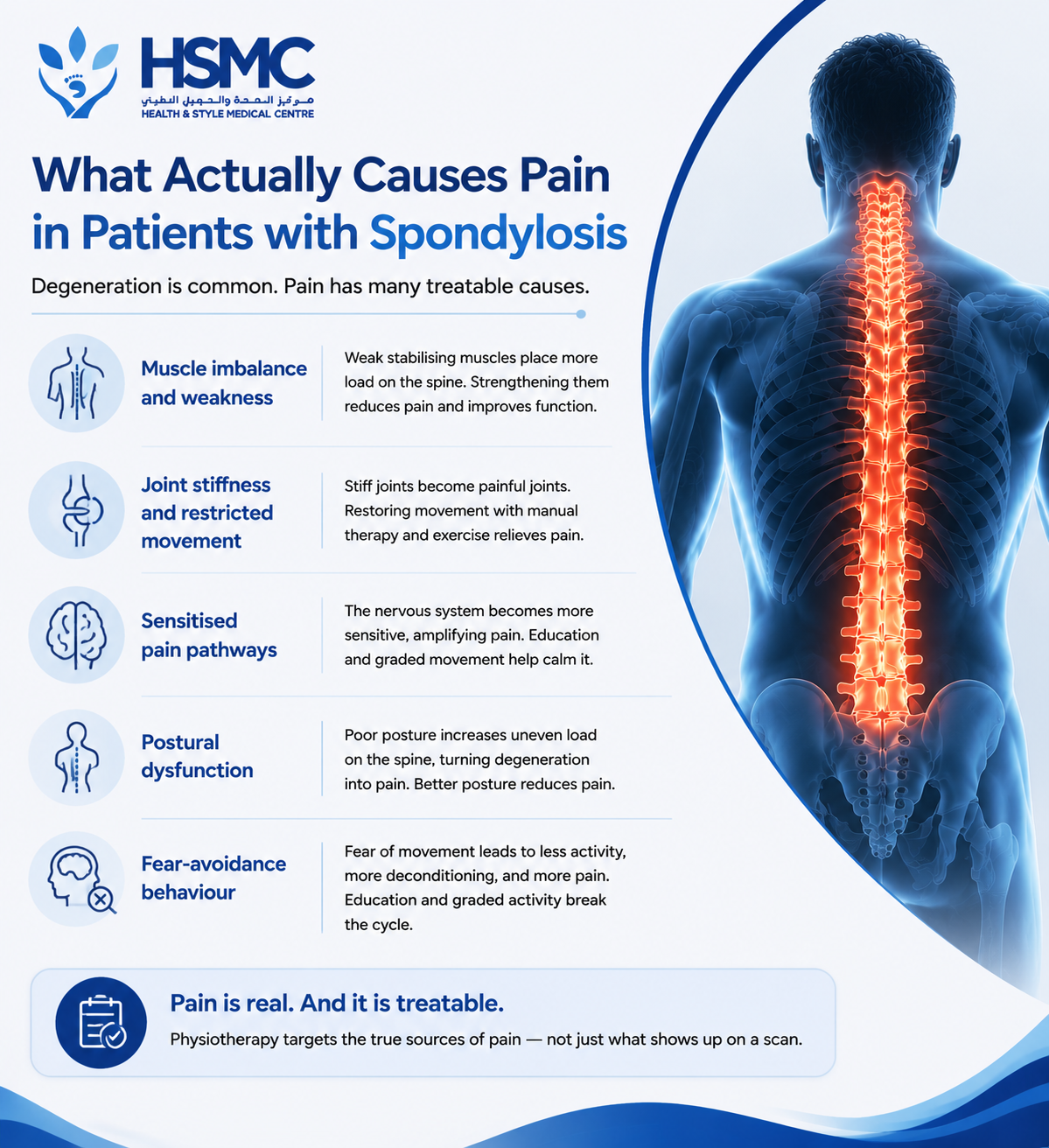
What Actually Causes Pain in Patients with Spondylosis
If degeneration is not directly causing pain in most cases, what is?
In our clinical experience, the pain experienced by patients with spondylosis typically arises
from one or more of the following treatable sources:
Muscle imbalance and weakness. As the spine ages and degenerates, the deep stabilising
muscles — the multifidus, transversus abdominis, and pelvic floor — often become inhibited
and weak. This leaves the degenerating structures under increased load, as they no longer
have the muscular support they depend on. Strengthening these muscles reduces pain and
improves function — regardless of what the scan shows.
Joint stiffness and restricted movement. Spondylotic changes reduce joint mobility, and
restricted joints become painful joints. Manual therapy and targeted exercise that restores
movement to stiff spinal segments often produces significant pain relief — even when the
underlying degeneration cannot be reversed.
Sensitised pain pathways. In chronic pain conditions, the nervous system itself becomes
more sensitive — amplifying pain signals that would otherwise be sub-threshold. This
central sensitisation is a major contributor to persistent pain in patients with spondylosis,
and it responds to specific pain education and graded movement approaches that
physiotherapy provides.
Postural dysfunction. Poor posture loads the degenerating structures asymmetrically and
excessively, converting a stable, non-painful degenerative process into a painful one.
Correcting the posture reduces the load and reduces the pain.
Fear-avoidance behaviour. The belief that movement will cause damage leads to reduced
activity, which leads to deconditioning, which leads to more pain, which confirms the belief.
Breaking this cycle through education and graded movement is one of physiotherapy’s most
powerful interventions.
What Physiotherapy Can Achieve for Spondylosis
Physiotherapy cannot reverse degenerative changes in the spine. Bone spurs will not
disappear. Lost disc height will not be restored. If your scan shows spondylosis, those
structural changes are there.
But here is what physiotherapy absolutely can do — and does, every day at Health & Style
Medical Centre:
Significantly reduce pain. Through manual therapy, exercise rehabilitation, and pain
education, most patients with spondylosis achieve meaningful and lasting pain reduction.
Many become effectively pain-free in daily life, even though their scan looks the same.
Restore movement and function. Joint mobilisation and progressive exercise rehabilitation
restore the mobility and strength that allow patients to return to activities they had given up
— whether that is walking comfortably, sleeping without pain, playing with their
grandchildren, or returning to sport.
Prevent deterioration. A strong, well-conditioned spine deteriorates more slowly than a
deconditioned one. Regular exercise and good movement habits slow the progression of
degenerative changes and reduce the risk of more serious problems developing.
Reduce reliance on medication. Many patients with spondylosis are managing their pain
with regular anti-inflammatory medication or stronger analgesics. Physiotherapy that
reduces pain at its source typically reduces — and in many cases eliminates — the need for
ongoing medication.
Improve quality of life. This is ultimately what matters most. Patients who commit to their
physiotherapy programme consistently report not just reduced pain but improved
confidence, better sleep, greater independence, and a restored ability to participate in the
activities that make their lives meaningful.
The Abu Dhabi Context
In Abu Dhabi, spondylosis is particularly common for several reasons. The combination of a
largely sedentary working population, extended daily sitting, limited outdoor movement
during the hot months, and a cultural tendency to seek imaging early and accept passive
diagnoses means that many residents are living unnecessarily limited lives with
undertreated spinal pain.
We also see significant numbers of patients from Abu Dhabi’s Arabic-speaking community
who have been told that their back pain is simply a consequence of age — and who have
accepted this with a resignation that is entirely unnecessary. Spondylosis is not a sentence.
It is a starting point for a conversation about what can be done.
When to Seek Further Medical Assessment
While physiotherapy is appropriate for the vast majority of patients with spondylosis, there
are situations where further medical assessment is warranted alongside physiotherapy
treatment:
- Significant neurological symptoms — weakness, widespread numbness, or bowel and bladder disturbance
- Severe spinal stenosis with limiting claudication (leg pain on walking that is relieved by sitting)
- Rapid or unexplained deterioration in symptoms
- Symptoms in younger patients (under 40) where inflammatory arthritis or other pathology should be excluded
Our physiotherapists are trained to identify these situations and to facilitate appropriate
medical referral when it is needed.

You Do Not Have to Accept the Pain
The message we want every Abu Dhabi patient with spondylosis to take from this article is
this: a scan showing degeneration is not a verdict. It is not permission to stop seeking help.
And it is absolutely not evidence that nothing can be done.
Physiotherapy does not cure spondylosis. But it can — and does — transform the lives of
people living with it.
Book your physiotherapy assessment at Health & Style Medical Centre, Abu Dhabi.

