

If you have ever woken up unable to reach behind your back to tuck in a shirt, been unable
to lift your arm above your head to take something from a shelf, or been stopped in your
tracks by a deep, aching shoulder pain that defies explanation — you may be one of the
many Abu Dhabi residents living with frozen shoulder.
Frozen shoulder — clinically known as adhesive capsulitis — is one of the most frustrating
and misunderstood conditions in musculoskeletal medicine. It is common, affecting approximately 2–5% of the general population. Significantly higher rates in people with diabetes and thyroid disorders — both conditions that are prevalent in the UAE. It is painful. It is functionally limiting. And it has a natural history that, in untreated or poorly treated patients, can stretch to two to three years of significant disability.
But here is what many Abu Dhabi patients with frozen shoulder do not know: with early,
correctly targeted physiotherapy, the duration and severity of the condition can be
substantially reduced. Patients who begin appropriate treatment in the early stages of
frozen shoulder — rather than waiting, as most do, until the condition is advanced — achieve
faster recovery, less severe functional limitation, and a significantly improved quality of life
throughout the process.
This article explains what frozen shoulder is, why patients in Abu Dhabi wait too long to seek
help, and how our physiotherapy approach addresses it effectively — often cutting recovery
timelines in half.
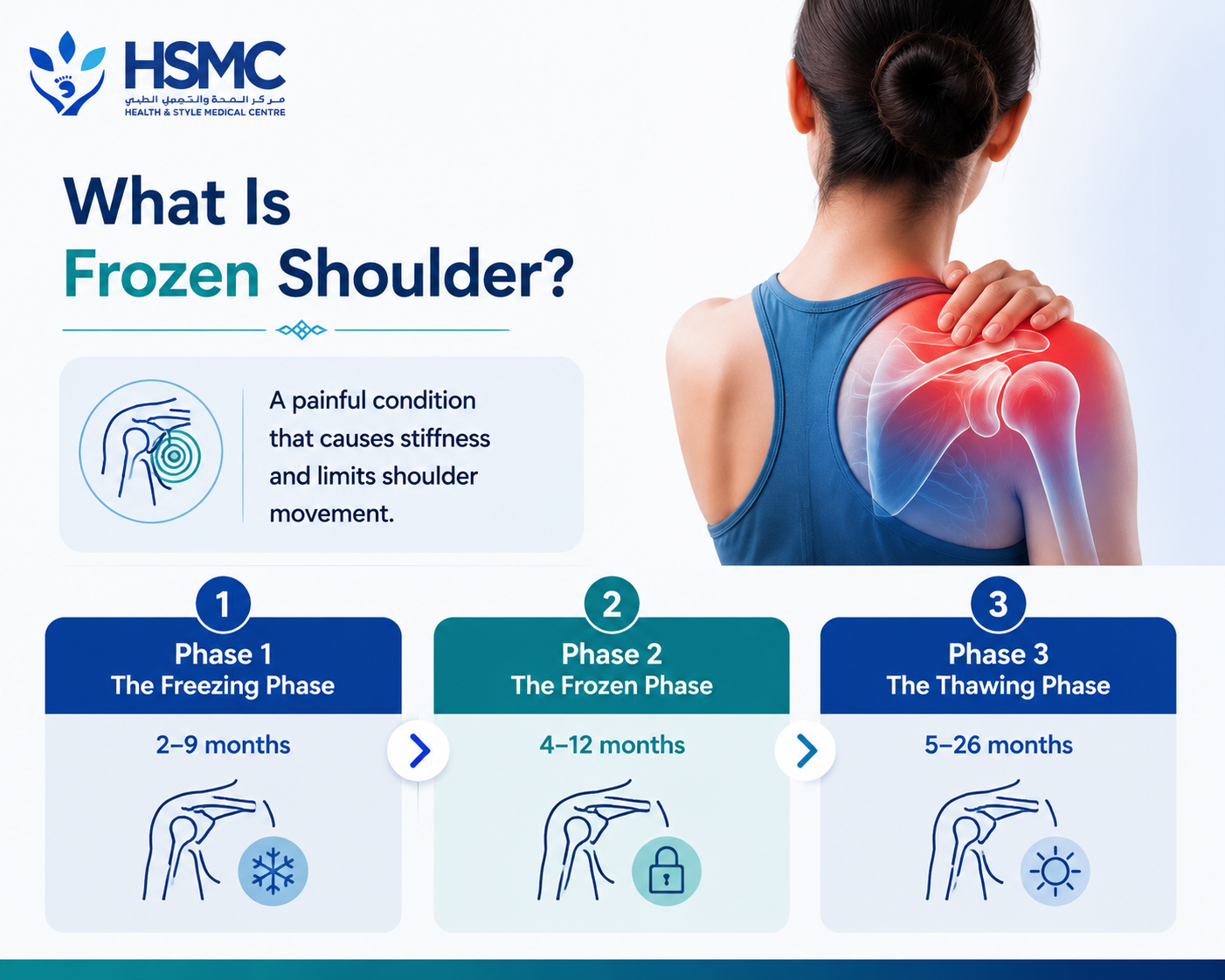
What Is Frozen Shoulder?
Frozen shoulder is a condition characterised by inflammation and thickening of the shoulder
joint capsule — the fibrous tissue envelope that surrounds and contains the glenohumeral
(ball-and-socket) shoulder joint. As the capsule becomes inflamed, it progressively
contracts and forms adhesions, significantly reducing the volume of the joint space and
restricting shoulder movement in all directions.
The condition progresses through three clinically recognisable phases:
Phase 1: The Freezing Phase (2–9 months)
The onset is typically gradual — a dull ache in the shoulder, initially attributed to a minor
strain or overuse, that progressively worsens over weeks to months. Night pain is
characteristic and often severe — waking the patient when they roll onto the affected
shoulder, or even disturbing sleep without positional change. Movement becomes
increasingly painful, and patients begin to notice that their shoulder range of motion is
reducing.
This is the phase in which intervention is most effective — and the phase in which most
patients either do not yet recognise the condition or are told to rest and wait.
Phase 2: The Frozen Phase (4–12 months)
Pain remains significant but may begin to plateau or reduce slightly as the acute
inflammatory process subsides. The dominant feature is now stiffness — a profound
restriction of shoulder movement in all planes, particularly external rotation and elevation.
Simple tasks — reaching overhead, fastening a bra, reaching into a back pocket, combing
the back of the hair — become difficult or impossible. This phase represents the peak of
functional disability.
Phase 3: The Thawing Phase (5–26 months)
The adhesions gradually loosen and the shoulder range of motion slowly returns. In patients
who have received appropriate physiotherapy, this phase is accelerated significantly. In
untreated patients, the thawing phase can extend for years — and some patients never
achieve full recovery without intervention.
Why Patients Wait Too Long
In our clinical experience at Health & Style Medical Centre, the average Abu Dhabi patient
with frozen shoulder presents for physiotherapy significantly later than the optimal
treatment window. Several factors contribute to this delay:
Misattribution to other causes. In the early freezing phase, frozen shoulder is easily
dismissed as a minor muscle strain, rotator cuff problem, or referred pain from the neck.
The gradual onset means the progressive nature of the condition is not immediately
apparent, and many patients wait for it to resolve on its own — which it does not.
Cultural stoicism. The tendency to endure musculoskeletal pain without seeking help —
particularly for conditions that do not prevent work or essential daily function — means that
many patients live with significant pain and restriction for months before presenting for
assessment.
Reliance on rest and medication. Anti-inflammatory medication provides partial and
temporary relief of frozen shoulder pain but does not address the capsular inflammation and
contracture that drive the condition. Patients who manage with painkillers for months are
delaying the treatment that would actually accelerate their recovery.
Misinformation about natural history. The belief that frozen shoulder “always resolves on
its own eventually” leads many patients to adopt a passive waiting approach. While it is true
that frozen shoulder has a natural history of eventual spontaneous resolution, this resolution
takes an average of 18–30 months in untreated patients — and is incomplete in a significant
proportion, with some degree of residual stiffness persisting permanently.
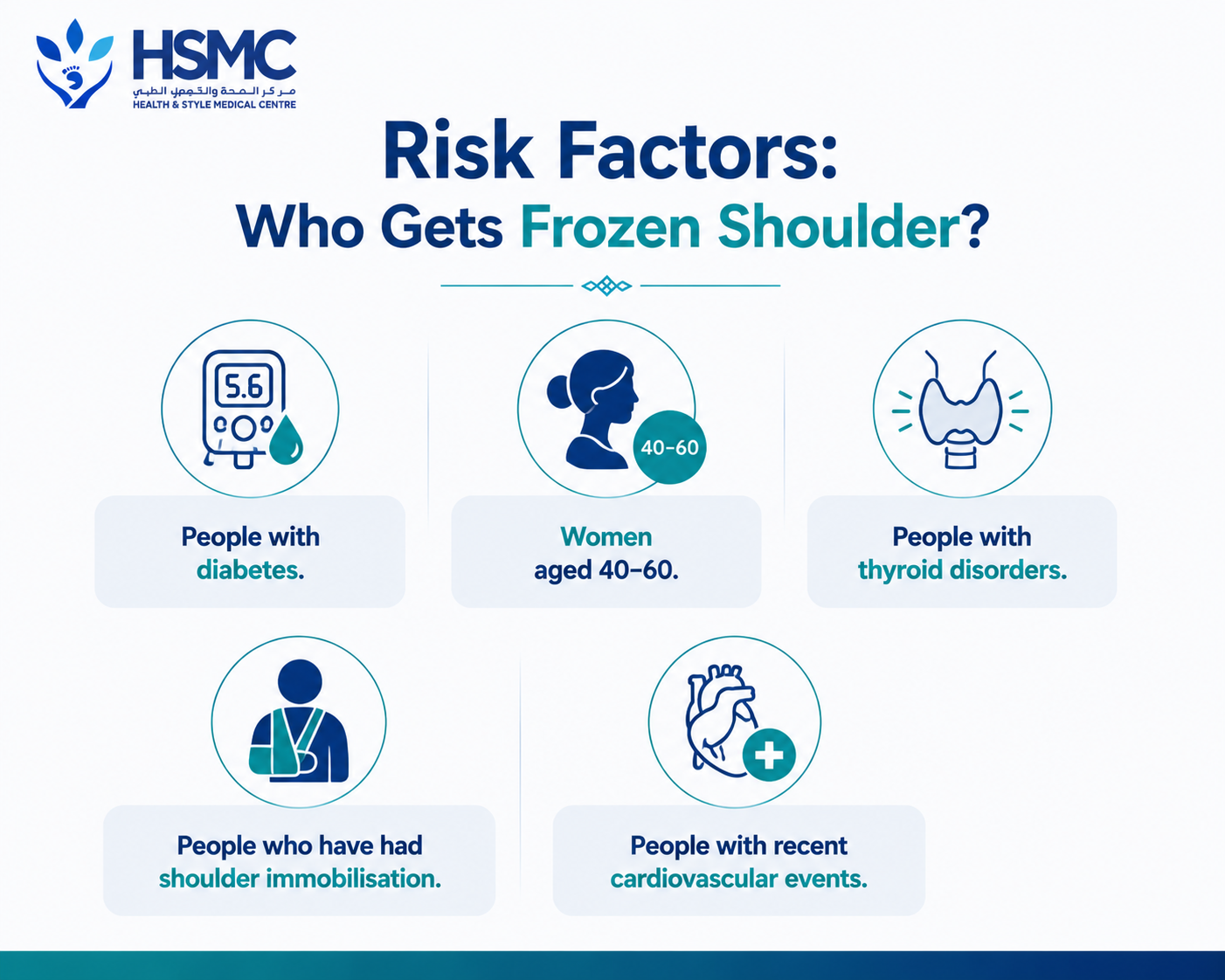
Risk Factors: Who Gets Frozen Shoulder?
Understanding who is at elevated risk helps with early identification and earlier treatment.
Frozen shoulder is significantly more common in:
People with diabetes. Diabetic frozen shoulder is more severe, more bilateral (affecting
both shoulders), more resistant to treatment, and more likely to recur than frozen shoulder
in the non-diabetic population. Given the UAE’s extremely high diabetes prevalence, this is a
clinically important risk group.
Women aged 40–60. Frozen shoulder has a well-established female predominance, with
peak incidence in perimenopausal and postmenopausal women — suggesting hormonal
influences on capsular tissue properties.
People with thyroid disorders. Both hypothyroidism and hyperthyroidism are associated
with elevated frozen shoulder risk.
People who have had shoulder immobilisation. Prolonged immobilisation following
shoulder injury, surgery, or upper limb fracture is a significant precipitating factor for
secondary frozen shoulder.
People with recent cardiovascular events. Frozen shoulder is associated with myocardial
infarction and stroke, both through immobilisation and through unclear neurogenic
mechanisms.

How We Treat Frozen Shoulder at Health & Style
The approach to frozen shoulder treatment has evolved significantly in recent years, and the
evidence now points clearly toward early, active physiotherapy as the most effective
management strategy — considerably more effective than the historically common
approach of waiting for the condition to progress before intervening.
Phase-specific treatment. The treatment approach is tailored to the phase of the
condition. Treating a freezing-phase patient with aggressive mobilisation is painful and
counterproductive — just as treating a frozen-phase patient with gentle rest is ineffective.
Our physiotherapists accurately stage each patient’s condition and match the treatment
intensity and approach accordingly.
Freezing phase treatment:
- Corticosteroid injection — where our physiotherapists work in collaboration with the treating physician or orthopedic surgeon, a targeted intra-articular steroid injection in the early freezing phase has strong evidence for reducing the duration and severity of the condition. Physiotherapy commenced shortly after injection produces significantly better outcomes than injection alone.
- Pain management — patient education, activity modification, and sleep positioning advice to reduce the impact of night pain
- Gentle, pain-free range of motion exercises — maintaining as much movement as possible without aggravating the inflammatory process
- Neural mobilization — addressing the neural tension that commonly accompanies frozen shoulder and contributes to pain
Frozen phase treatment:
- Progressive joint mobilisation — hands-on techniques targeting the inferior and posterior capsular restrictions that are the primary mechanical drivers of the stiffness.
- High-grade mobilisation in the frozen phase has strong evidence for accelerating range of motion recovery.
- Capsular stretching — sustained, progressive stretching of the contracted capsule in specific directions — particularly into external rotation and elevation — is the cornerstone of range of motion recovery in this phase
- Strengthening — as movement returns, progressive strengthening of the rotator cuff and scapular stabilisers prevents the secondary weakness and instability that develop during the frozen phase
- Home exercise programme — the daily stretching and mobility work performed by the patient between sessions is as important as the in-clinic treatment. Recovery from frozen shoulder is a partnership — patients who perform their home programme diligently recover significantly faster than those who rely solely on clinic sessions.
Thawing phase treatment:
- Progressive strengthening and functional rehabilitation — restoring the full muscle capacity of the shoulder and returning to all desired activities
- Sport or work-specific rehabilitation where relevant
Hydrodilatation and Surgical Options
For patients whose frozen shoulder does not respond adequately to physiotherapy and
injection, two further options are available:
Hydrodilatation (distension arthrography). A radiologist injects fluid into the joint capsule
under imaging guidance, stretching and rupturing the adhesions. This can produce rapid
improvement in range of motion and is followed by intensive physiotherapy to consolidate
and build on the gains.
Manipulation under anaesthesia (MUA) or arthroscopic capsular release. Surgical
options for frozen shoulder that has not responded to conservative management. Our
physiotherapists liaise with orthopaedic surgeons regarding appropriate timing and facilitate
pre- and post-procedural rehabilitation.
The Half-Time Recovery Promise
Our experience at Health & Style Medical Centre consistently demonstrates that patients
who begin physiotherapy in the early to mid-freezing phase — rather than waiting until the
full frozen phase — achieve clinical resolution in substantially less time than the natural
history would suggest. Where untreated frozen shoulder takes 18–30 months to resolve
spontaneously, patients who engage early with evidence-based physiotherapy typically
achieve excellent functional recovery in 3–6 months.
That difference — 18–30 months versus 3–6 months — represents more than a year of
unnecessary pain, functional limitation, disrupted sleep, and reduced quality of life.
Do not wait. If your shoulder has been aching and stiffening for more than a few weeks
without clear explanation, seek assessment now.
Book your shoulder assessment at Health & Style Medical Centre, Abu Dhabi.
- Tags:
- Frozen Shoulder

