

For patients whose hip has been destroyed by osteoarthritis — whose every step has
become an exercise in pain management, whose sleep has been disrupted for months by a
joint that never stops complaining, whose world has contracted to the distance they can
walk before the pain becomes unbearable — total hip replacement is often genuinely
transformative.
The surgery replaces the damaged hip joint with a prosthetic implant, eliminating the bone
on-bone friction that causes the pain and restoring a smooth, functional joint surface. For
the majority of patients, the results are remarkable — a dramatic reduction in pain that
begins almost immediately after surgery and a progressive return to function that, with the
right rehabilitation, allows most patients to walk normally, climb stairs, drive, and return to
the activities they had given up.
But the speed and completeness of that recovery are not fixed by the surgery. They are
determined, in large measure, by how early, how expertly, and how consistently
rehabilitation begins.
At Health & Style Medical Centre, we are committed to getting Abu Dhabi’s hip replacement
patients walking again — sooner, more confidently, and more completely than they might
achieve with less specialised post-surgical support. This article explains how we do it.
Why Hip Replacement Rehabilitation Requires Expert Guidance
Hip replacement rehabilitation is not simply a matter of progressively increasing walking
distance. It involves understanding the specific surgical approach used, respecting the hip
precautions that protect the new implant during healing, managing the complex
neuromuscular recovery that follows major joint surgery, and progressing the patient
systematically through a rehabilitation programme designed for their individual
circumstances.
The surgical approach matters. Hip replacement can be performed through several
different surgical approaches — posterior, anterolateral, direct anterior, and lateral — each
of which involves different soft tissue dissection and creates different precaution
requirements and rehabilitation considerations. Our physiotherapists are familiar with all
major surgical approaches and tailor rehabilitation accordingly.
Hip precautions protect the implant. In the early post-operative period, the replaced hip
is at risk of dislocation — the femoral head component can be displaced from the acetabular
cup component if the hip is moved into certain positions before the surrounding soft tissues
have healed and regained their tensioning function.
For the traditional posterior approach, the standard hip precautions are: avoid hip flexion
beyond 90 degrees, avoid adduction (crossing the legs), and avoid internal rotation.
Violation of these precautions risks dislocation — a serious complication requiring
emergency medical attention and, in some cases, revision surgery.
For the direct anterior approach — increasingly popular because it involves less soft tissue
dissection and potentially faster recovery — precautions are typically less restrictive. Your
physiotherapist will know precisely which precautions apply based on the surgical report
from your surgeon.
Understanding and teaching these precautions — ensuring that every movement the patient
makes, in the clinic and at home, respects the relevant restrictions — is one of the most
important early responsibilities of the post-surgical physiotherapist.
The Recovery Timeline
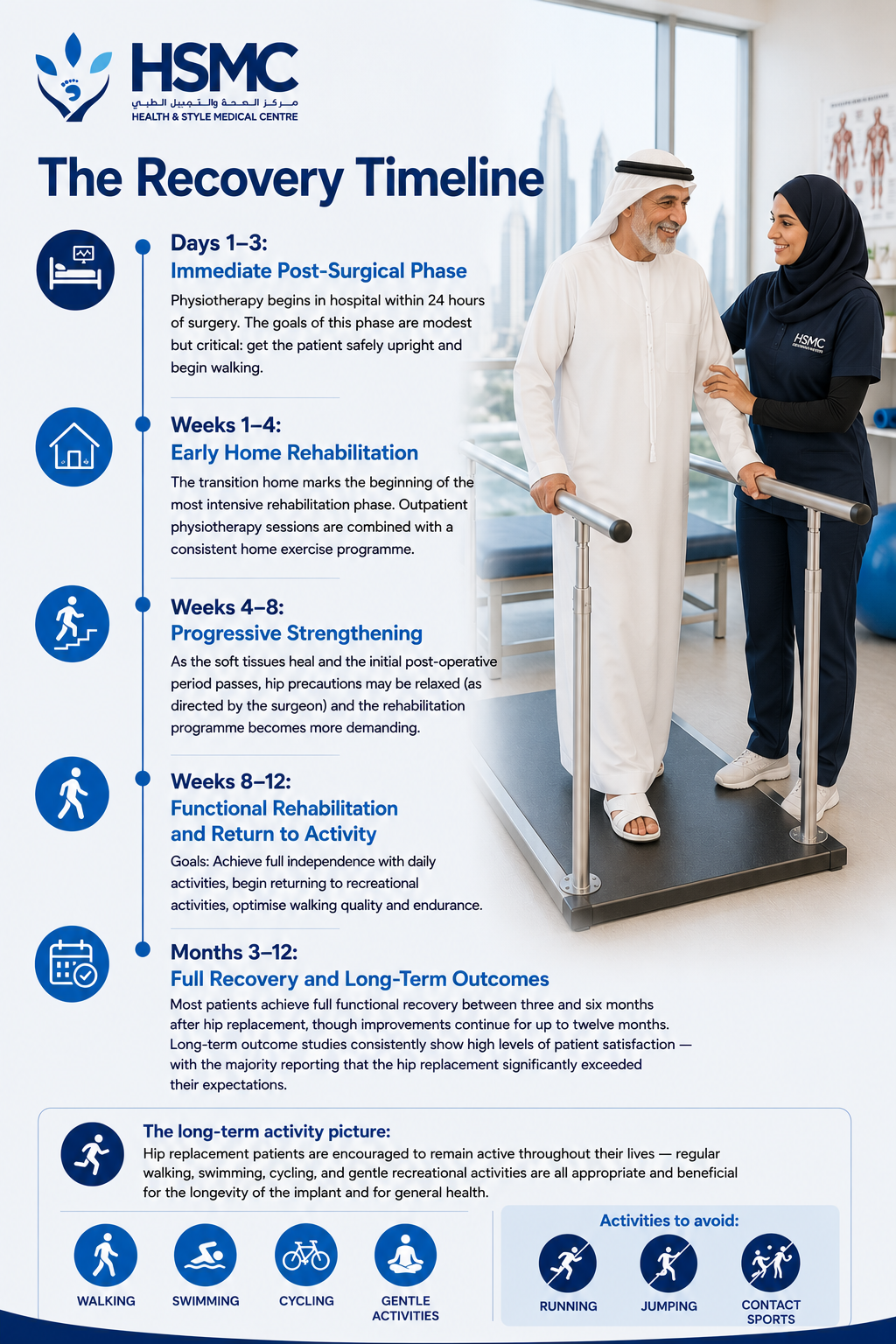
Days 1–3: Immediate Post-Surgical Phase
Physiotherapy begins in hospital within 24 hours of surgery. The goals of this phase are
modest but critical: get the patient safely upright and begin walking.
Key interventions:
- Bed exercises — ankle pumps, quadriceps sets, gluteal sets, and gentle heel slides
- within the permitted range
- Assisted transfer from bed to chair — practising the technique that maintains hip
- precautions throughout
- Initial walking with a walking frame or crutches, with weight-bearing on the operated leg
- as directed by the surgeon
- Education on hip precautions and their practical application in every daily activity
The hip precautions in daily life: Every activity in the early phase of hip replacement
recovery must be performed in a way that respects the hip precautions. Getting in and out
of bed, sitting down and standing up, using the toilet, showering, dressing — all require
specific techniques that our physiotherapists teach and reinforce until they become
automatic. This functional education is as important as the exercise programme.
Weeks 1–4: Early Home Rehabilitation
The transition home marks the beginning of the most intensive rehabilitation phase.
Outpatient physiotherapy sessions are combined with a consistent home exercise
programme.
Goals: Master hip-safe movement techniques, achieve safe independent mobility, reduce
pain and swelling, begin progressive strengthening.
Key physiotherapy interventions:
- Hip-safe sit-to-stand, bed transfers, and daily activity techniques — reinforced and refined at every session
- Progressive walking — increasing distance and confidence, transitioning from walking frame to crutches to a single stick as strength and balance allow
- Strengthening exercises within permitted range — gluteal sets, hip abductor strengthening in side-lying, inner range quadriceps, terminal knee extension
- Swelling management — elevation, ice, and compression
- Stair training — initially one step at a time (leading with the non-operated leg going up, operated leg going down), progressing as strength and confidence improve
- Falls prevention — particularly important in the early phase when balance and strength are compromised and the consequence of a fall includes potential dislocation or periprosthetic fracture
What to expect: The first two to four weeks after hip replacement are demanding. Pain,
fatigue, and the cognitive load of remembering and implementing hip precautions
simultaneously makes this period tiring even for patients who are progressing well. Most
patients achieve independence with daily activities within three to four weeks — though they
continue to need walking aids for outdoor mobility.
Weeks 4–8: Progressive Strengthening
As the soft tissues heal and the initial post-operative period passes, hip precautions may be
relaxed (as directed by the surgeon) and the rehabilitation programme becomes more
demanding.
Goals: Wean from walking aids, improve gait quality, build hip and lower limb strength,
improve balance and proprioception.
Key physiotherapy interventions:
- Progressive hip and lower limb strengthening — hip abductor, hip extensor, and quadriceps strengthening form the core of this phase. The gluteus medius — the primary lateral stabiliser of the pelvis during walking — is particularly critical. Weakness here produces the characteristic Trendelenburg gait (hip drop to the opposite side) that persists after hip replacement when rehabilitation is inadequate
- Gait retraining — correcting the antalgic gait patterns (compensatory movement strategies) that patients develop over months or years of painful walking and that can persist after surgery if not specifically addressed
- Balance and proprioceptive training — the hip joint is rich in mechanoreceptors that are disrupted by surgery; proprioceptive retraining rebuilds the position sense and balance control that normal hip function requires
- Stationary cycling — an excellent tool for restoring hip range of motion and building lower limb strength at this stage
- Hydrotherapy where available — water-based exercise at four to six weeks post-surgery (once the wound has fully healed) provides an excellent environment for rebuilding movement confidence and strength with reduced loading
What to expect: Significant and visible improvement in walking quality, endurance, and
confidence. Most patients are walking without aids indoors and progressing toward outdoor
independence. The hip will still feel different — awareness of the implant, occasional clicking
or clunking, and some residual swelling are all normal at this stage.
Weeks 8–12: Functional Rehabilitation and Return to Activity
Goals: Achieve full independence with daily activities, begin returning to recreational
activities, optimise walking quality and endurance.
Key physiotherapy interventions:
- Advanced strengthening — single-leg exercises, progressive resistance training
- targeting the hip and gluteal muscles
- Functional movement training — walking on uneven terrain, inclines, steps of varying
- heights, and in community environments
- Return to driving assessment — most patients can return to driving at six to eight weeks
- if the right hip has been operated on and an automatic vehicle is used, subject to
- surgeon clearance
- Return to recreational activity — walking programmes, swimming, cycling, and golf are
- typically introduced in a graduated fashion during this phase
Months 3–12: Full Recovery and Long-Term Outcomes
Most patients achieve full functional recovery between three and six months after hip
replacement, though improvements continue for up to twelve months. Long-term outcome
studies consistently show high levels of patient satisfaction — with the majority reporting
that the hip replacement significantly exceeded their expectations.
The long-term activity picture: Hip replacement patients are encouraged to remain active
throughout their lives — regular walking, swimming, cycling, and gentle recreational
activities are all appropriate and beneficial for the longevity of the implant and for general
health. High-impact activities — running, jumping, contact sports — are generally
discouraged to protect implant longevity.
Why Starting Early Makes Such a Difference

At Health & Style Medical Centre, we see a consistent pattern: patients who begin
outpatient physiotherapy within the first week of hospital discharge achieve better range of
motion, stronger muscles, and superior gait quality at every subsequent timepoint
compared to those who delay.
The reasons are multiple. Early physiotherapy prevents the development of scar tissue
adhesions that restrict movement. It maintains and builds muscle strength before significant
deconditioning sets in. It corrects compensatory movement patterns before they become
habitual. And it provides the expert guidance that ensures every stage of the recovery
process is navigated optimally.
Hip replacement is a significant surgical investment. Expert physiotherapy rehabilitation is
what realises the full value of that investment.
Book your hip replacement rehabilitation assessment at Health & Style Medical
Centre, Abu Dhabi.

