

The UAE has one of the highest rates of diabetes in the world. According to the International
Diabetes Federation, approximately 17% of UAE adults aged 20–79 live with diabetes — one
of the highest national prevalences globally, and a figure that places an enormous burden
on the country’s healthcare system and on the individuals and families affected.
Among the most serious and most preventable complications of diabetes are those
affecting the feet. Diabetic foot problems — encompassing peripheral neuropathy,
peripheral vascular disease, foot deformity, ulceration, and in severe cases, amputation —
represent a significant source of disability, hospitalization, and reduced quality of life for
people with diabetes across the UAE.
What is less widely understood is the role that physiotherapy plays in the long-term
management of diabetic foot health. Physiotherapy does not simply treat injuries that have
already occurred — it prevents them. It addresses the biomechanical, neuromuscular, and
vascular factors that elevate risk, protects the foot from the cumulative damage that leads
to ulceration, and supports the broader physical health of people living with diabetes.
This article explains the mechanisms behind diabetic foot problems, the specific risks facing
people with diabetes in Abu Dhabi, and how physiotherapy forms an essential component of
comprehensive diabetic foot management.
Why Diabetes Is So Dangerous for the Feet

Diabetes affects the feet through several mechanisms that interact and compound each
other, creating a risk environment in which relatively minor injuries can escalate rapidly to
serious, life-threatening complications.
Peripheral neuropathy. Persistently elevated blood glucose levels damage the peripheral
nerves — the nerves that supply sensation, motor function, and autonomic regulation to the
feet and lower legs. Peripheral neuropathy affects approximately 50% of people who have
had diabetes for more than 25 years, and is present in many patients at the time of
diagnosis.
The consequences of peripheral neuropathy for the foot are profound:
Sensory neuropathy removes the foot’s warning system. Pain — the signal that tells us
something is wrong — is diminished or absent. A blister, a cut, a pressure sore, an ingrown
toenail — injuries that a person without neuropathy would notice and treat immediately — go
undetected in the diabetic foot. By the time the problem becomes visible, significant tissue
damage may already have occurred.
Motor neuropathy weakens the intrinsic muscles of the foot — the small muscles that
control the alignment and function of the toes and the arch. As these muscles weaken, the
toes develop deformities — claw toes, hammer toes — and the distribution of pressure
across the sole of the foot changes. Pressure concentrates at specific sites — the
metatarsal heads, the heel, the tips of deformed toes — creating the high-pressure zones
where ulceration most commonly develops.
Autonomic neuropathy reduces sweating in the foot, causing the skin to become dry,
cracked, and fragile — a further portal for infection entry.
Peripheral vascular disease. Diabetes accelerates atherosclerosis — the build-up of fatty
plaques in the walls of blood vessels. In the feet and lower legs, reduced blood flow means
that the tissues are less well-oxygenated, less able to resist infection, and less capable of
healing when injured. Even a small wound in a foot with compromised blood supply may fail
to heal — and can deteriorate into a chronic, infected ulcer.
Immune dysfunction. Elevated blood glucose impairs the function of the immune system —
reducing the white blood cells’ ability to fight infection. This means that infections in the
diabetic foot progress more rapidly, are harder to treat, and carry a higher risk of spreading
to bone (osteomyelitis) than in people without diabetes.
The diabetic foot ulcer cascade. The interaction of neuropathy, vascular disease, immune
dysfunction, and mechanical pressure creates the conditions for the diabetic foot ulcer — a
chronic wound that, once established, is the pathway to the most serious complications.
Approximately 15–25% of people with diabetes will develop a foot ulcer during their lifetime.
Of those who develop an ulcer, approximately 14–24% will ultimately require amputation.
These statistics are sobering. They are also, in large part, preventable
Several features of life in Abu Dhabi amplify the diabetic foot risk for UAE residents:
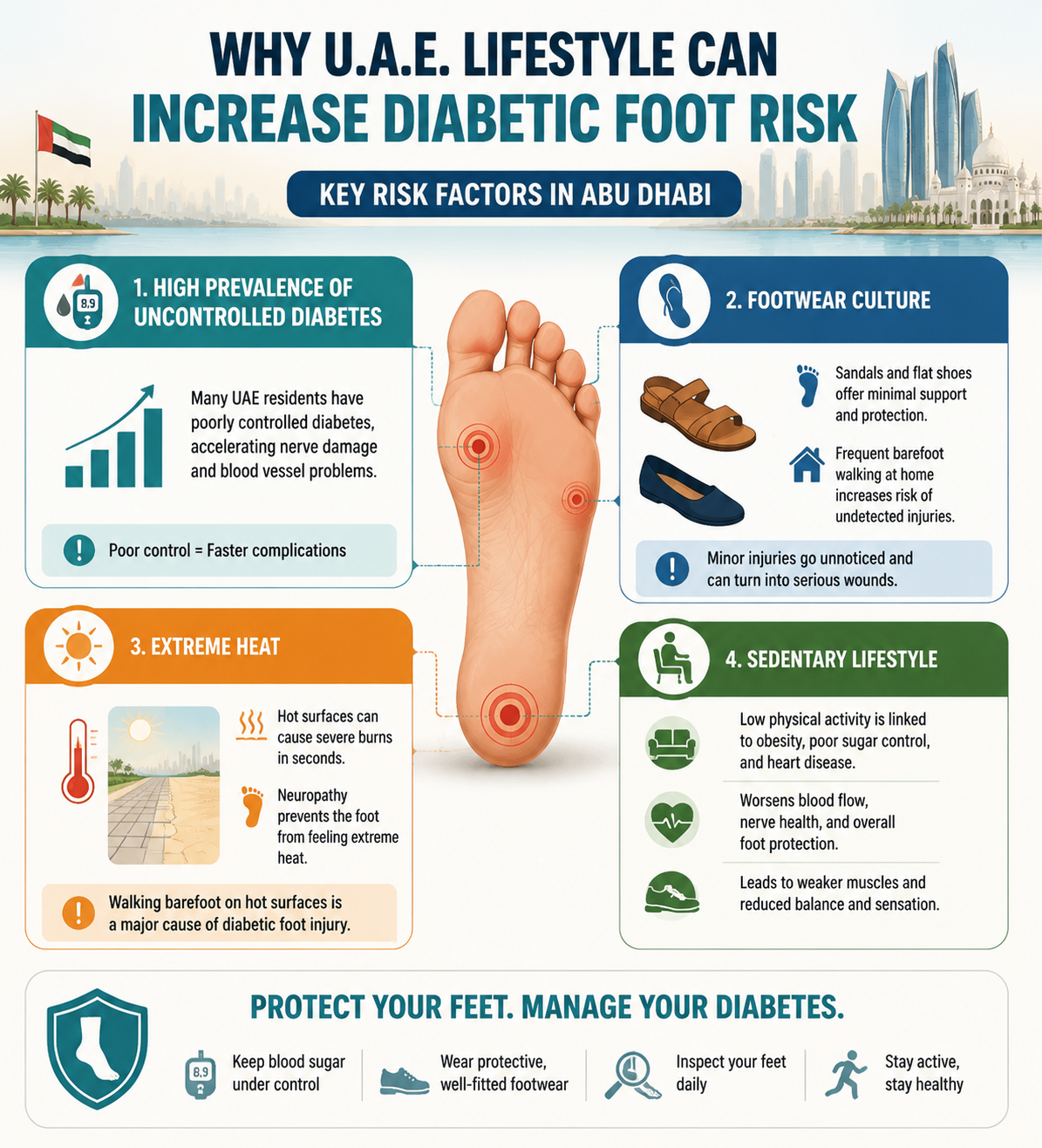
High prevalence of uncontrolled diabetes. The UAE’s diabetes epidemic is not simply one
of high prevalence — it is compounded by significant rates of poor glycaemic control. Many
UAE residents live with diabetes that is inadequately managed, accelerating the
development of neuropathy and vascular complications.
Footwear culture. Traditional footwear in the UAE — sandals and flat shoes that provide
minimal structural support — and the frequency of barefoot walking within the home creates
mechanical risk for feet that have lost protective sensation. A small stone, an uneven floor
tile, or the edge of a mat that would be immediately felt and avoided by a person with
normal sensation goes unnoticed in the neuropathic foot.
Heat. Abu Dhabi’s extreme heat creates specific risks for the diabetic foot. Hot surfaces —
sun-heated pavement, sand, tiles in direct sunlight — that would be immediately painful and
avoided by a person with normal sensation can cause serious thermal burns to neuropathic
feet in seconds. Walking barefoot on hot surfaces is one of the most common mechanisms
of serious diabetic foot injury.
Sedentary lifestyle. Physical inactivity is both a risk factor for developing type 2 diabetes
and a complication of its consequences. Painful neuropathy, reduced exercise tolerance
from cardiovascular disease, and obesity all reduce physical activity — which in turn
worsens glycaemic control, accelerates vascular disease, and reduces the muscular
strength and proprioception that protect the feet.
How Physiotherapy Addresses Diabetic Foot Risk
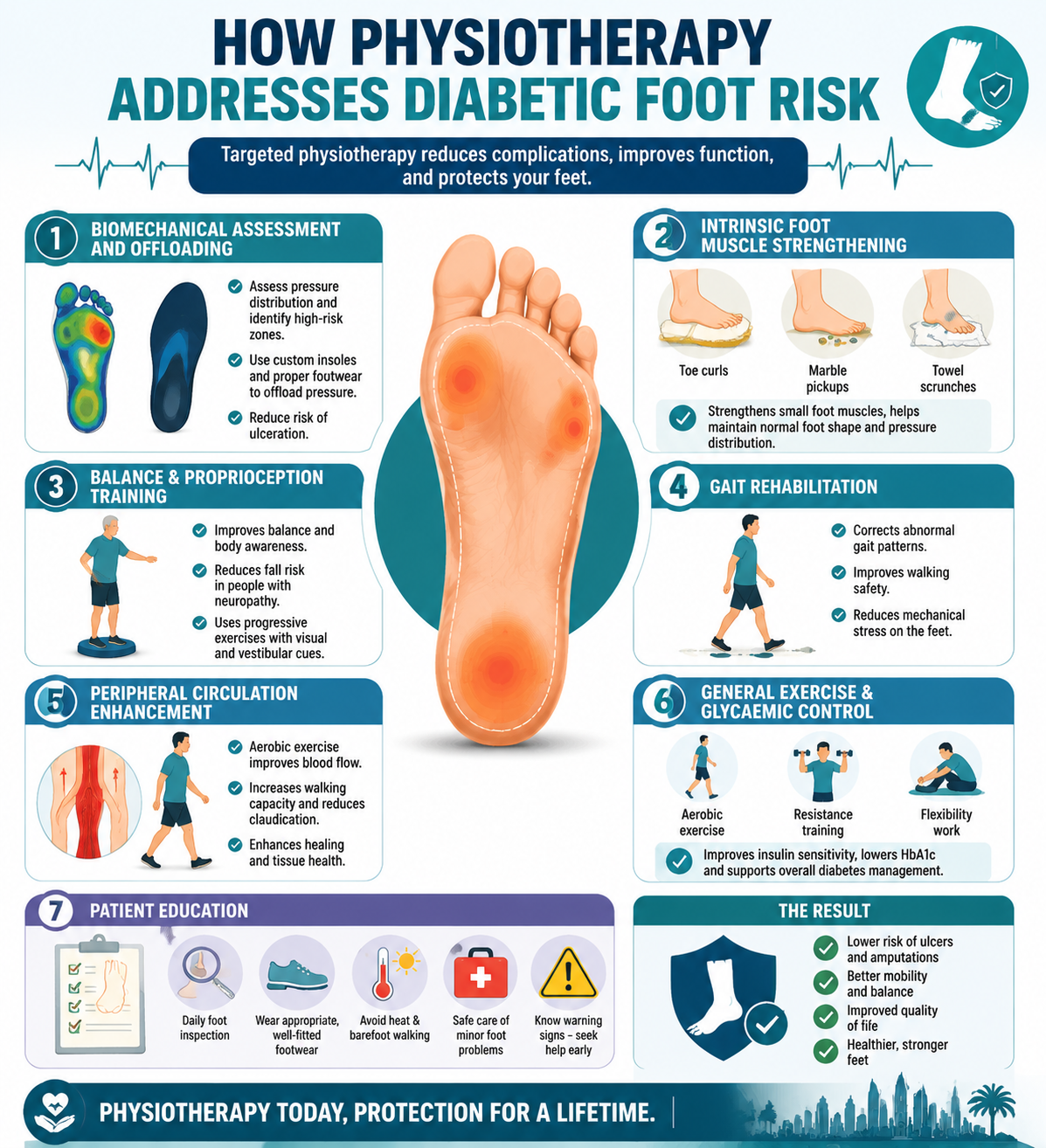
Biomechanical assessment and offloading. Our physiotherapists assess the distribution
of pressure across the sole of the foot — identifying the high-pressure zones that are most
at risk of ulceration — and design interventions to reduce this pressure. This may include
custom or semi-custom orthotic insoles that redistribute load away from vulnerable sites,
footwear assessment and recommendations, and specific exercises to address the toe
deformities and gait abnormalities that create localised high-pressure zones.
Intrinsic foot muscle strengthening. The motor neuropathy-related weakening of the
intrinsic foot muscles is a key driver of the toe deformities and altered pressure distribution
that precede ulceration. Targeted strengthening of these muscles — toe curls, marble
pickups, towel scrunches, and short foot exercises — partially offsets this weakness and
helps maintain a more normal foot architecture.
Balance and proprioception training. Sensory neuropathy profoundly impairs the
proprioceptive input from the feet that contributes to balance control. People with diabetic
peripheral neuropathy have significantly elevated fall risk — and falls carry serious
consequences when the feet and legs cannot heal effectively. Our balance training
programme progressively challenges proprioceptive and balance systems, incorporating
visual and vestibular cues to compensate for reduced somatosensory input from the feet.
Gait rehabilitation. Altered gait patterns in people with diabetic neuropathy — the wide
based, slow, shuffling walk that characterises advanced peripheral neuropathy — increase
fall risk and create abnormal mechanical loading of the foot. Gait retraining improves
walking safety, reduces fall risk, and may reduce the mechanical stress on at-risk foot
regions.
Peripheral circulation enhancement. Aerobic exercise is the most evidence-based
intervention for improving peripheral circulation in people with peripheral vascular disease.
Even moderate-intensity walking programmes significantly improve claudication distance
and functional walking capacity in people with diabetes-related peripheral vascular disease.
Our physiotherapists design safe, progressive aerobic exercise programmes that improve
peripheral perfusion without exceeding the patient’s cardiovascular capacity.
General exercise and glycaemic control. Physical activity is one of the most powerful
tools for improving blood glucose control in type 2 diabetes. Regular exercise increases
insulin sensitivity, reduces HbA1c, and directly addresses the primary metabolic driver of all
diabetic complications. Our physiotherapy team provides comprehensive exercise
programming — combining aerobic exercise, resistance training, and flexibility work — that
optimises glycaemic control as part of the overall diabetes management strategy.
Patient education. Education is a cornerstone of diabetic foot management. Our
physiotherapists provide detailed guidance on daily foot inspection, appropriate footwear,
safe management of minor foot problems, the specific hazards of Abu Dhabi’s heat and
barefoot culture, and the warning signs that require prompt medical attention.
The Diabetic Foot Care Team
Effective diabetic foot management is a multidisciplinary endeavour. Physiotherapy works
most effectively as part of a coordinated team that includes the patient’s endocrinologist or
diabetologist, a podiatrist, a vascular surgeon, and — when wounds are present — a wound
care specialist.
At Health & Style Medical Centre, our physiotherapy team communicates actively with the
other healthcare providers involved in our patients’ diabetes management, ensuring that the
exercise and rehabilitation programme we provide is aligned with the broader management
plan and that any concerns identified during physiotherapy are communicated promptly to
the appropriate specialists.
The Prevention Imperative
The most powerful message in diabetic foot management is this: prevention is
immeasurably more effective — and less costly in every sense — than treatment of
established complications.
A physiotherapy programme that maintains foot muscle strength, improves balance,
optimises footwear, enhances peripheral circulation, and keeps the patient physically active
does not simply improve quality of life in the short term. It reduces the probability of the
ulcer that leads to the hospitalisation. It reduces the probability of the fall that leads to the
hip fracture. It reduces the probability of the amputation that changes a life forever.
For people with diabetes in Abu Dhabi — a city with one of the world’s highest diabetes
prevalences — physiotherapy is not an optional extra. It is an essential component of the
long-term management strategy that protects health, independence, and quality of life.
Book your diabetic foot physiotherapy assessment at Health & Style Medical Centre,
Abu Dhabi.
- Tags:
- foot care
- Plantar fasciitis

