


Total knee replacement is one of the most commonly performed orthopedic procedures in
the world — and one of the most consistently effective. For patients whose knee
osteoarthritis has progressed to the point where pain is constant, function is severely
limited, and conservative management has been exhausted, knee replacement surgery
offers the prospect of a dramatic improvement in quality of life.
But the surgery itself is only half of the equation. What happens in the weeks and months
after the operation — the rehabilitation — determines how fully and how quickly that
improvement is realized. The difference between a patient who achieves an excellent
outcome and one who achieves a mediocre one is rarely the surgery. It is almost always the
rehabilitation.
In Abu Dhabi, where the number of knee replacement surgeries performed annually
continues to grow alongside the ageing population and the high prevalence of obesity —
both major risk factors for knee osteoarthritis — post-surgical physiotherapy rehabilitation is
a clinical service of increasing importance. And yet many patients receive inadequate
rehabilitation guidance, are discharged from hospital with a basic exercise sheet and
insufficient physiotherapy support, and achieve outcomes well below what their surgery
made possible.
This article provides a complete, week-by-week guide to total knee replacement
rehabilitation — what to expect at each stage, what physiotherapy achieves, and why the
commitment to rehabilitation is the most important investment a knee replacement patient
can make
Understanding Total Knee Replacement
Total knee replacement (TKR) — also called total knee arthroplasty — involves removing the
damaged surfaces of the femur (thigh bone), tibia (shin bone), and sometimes the patella
(kneecap), and replacing them with artificial components typically made of metal alloys and
high-density polyethylene. The result is a smooth, pain-free articulating surface that
restores the mechanical function the arthritic joint had lost.
Modern knee replacements are highly durable — the majority last 15–20 years or more with
appropriate care — and the surgical techniques have been refined to produce consistent,
reproducible results. The limiting factor on outcomes is not the implant. It is the
rehabilitation.
Before Surgery: The Case for Prehabilitation
The rehabilitation process does not begin on the day of surgery. It begins weeks before —
and patients who invest in pre-surgical physiotherapy (prehabilitation) consistently achieve
better post-surgical outcomes than those who do not.
Prehabilitation for total knee replacement focuses on:
Quadriceps strengthening. The quadriceps muscles are profoundly inhibited after knee
replacement surgery — a consequence of the arthrogenic muscle inhibition (AMI) that
surgery triggers, combined with the pain and swelling of the immediate post-operative
period. Patients who arrive at surgery with stronger quadriceps recover this strength faster
and achieve better early functional outcomes.
Hip strengthening. The gluteal muscles and hip abductors play a critical role in knee
alignment and function during rehabilitation exercises. Strengthening these muscles before
surgery reduces the work required to reestablish neuromuscular control after the
procedure.
Range of motion optimisation. Achieving the maximum possible knee flexion and
extension before surgery gives the post-operative rehabilitation the best possible starting
point.
Cardiovascular conditioning. General physical fitness improves surgical outcomes,
reduces complication risk, and supports the demanding rehabilitation process that follows.
Education and expectation setting. Patients who understand what to expect at each stage
of recovery — what will be difficult, what progress looks like, and what their role in
rehabilitation is — navigate the process with significantly less anxiety and greater
compliance.
If you are scheduled for knee replacement in Abu Dhabi and have not yet been referred for
prehabilitation physiotherapy, ask your surgeon to arrange it. The evidence supporting its
value is strong.
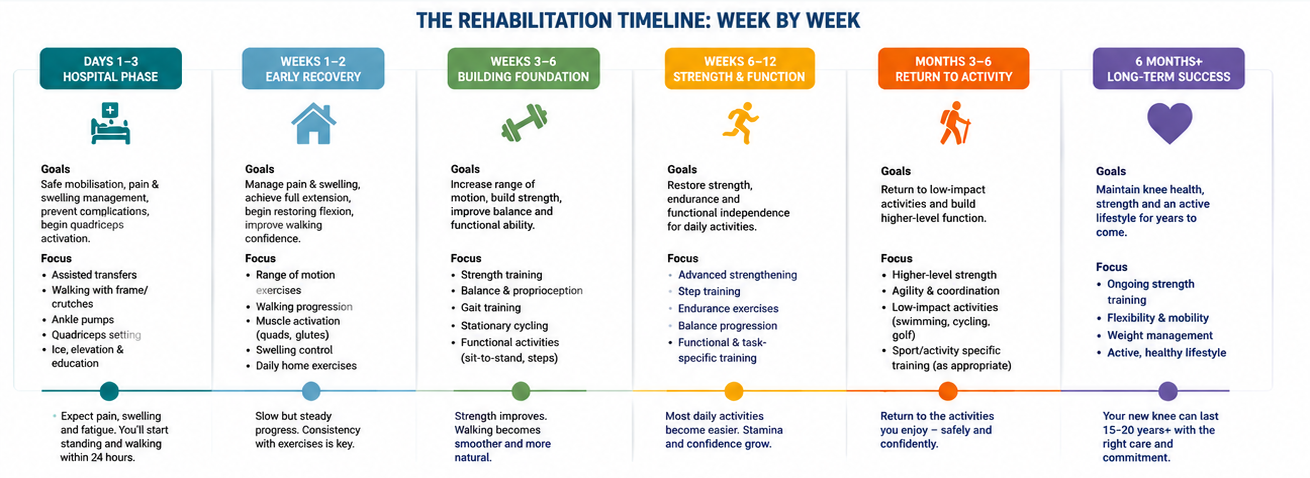
The Rehabilitation Timeline: Week by Week
Days 1–3: Hospital Phase
Physiotherapy begins on the day of surgery or the following day — while the patient is still in
hospital. This immediacy is not optional. Early mobilisation is essential for reducing
complication risk and initiating the neurological recovery process.
Goals: Safe mobilisation, pain and swelling management, prevent complications, begin
quadriceps activation.
Key physiotherapy interventions:
- Assisted transfer from bed to chair and initial standing
- Gait training with a walking frame or crutches — weight-bearing as tolerated on the
- operated leg
- Ankle pumps and calf raises to reduce DVT risk
- Quadriceps setting exercises — isometric contractions to begin reactivating the
- inhibited quadriceps
- Ice and elevation to manage swelling
- Education about post-discharge exercises and activity expectations
What to expect: Significant pain, swelling, and fatigue. The knee will feel unfamiliar and the
range of motion will be limited. Early mobilisation is uncomfortable but essential — and most
patients are surprised to find they can stand and begin walking within 24 hours of surgery.
Weeks 1–2: Early Home Recovery
After discharge — typically two to four days after surgery — rehabilitation continues at home
and in outpatient physiotherapy sessions.
Goals: Manage pain and swelling, achieve full knee extension, begin restoring knee flexion,
improve walking confidence.
Key physiotherapy interventions:
- Continuation of hospital exercises with increasing repetitions and challenge
- Passive and active-assisted knee extension — achieving and maintaining full extension is
- a critical early goal. Extension deficit is associated with gait abnormalities, ongoing pain,
- and poor long-term outcomes
- Progressive knee flexion exercises — heel slides, gravity-assisted flexion
- Straight leg raises — building quadriceps strength without loading the healing joint
- Gait training — progressing from walking frame to crutches as confidence and strength
- allow
- Ice and elevation protocols to manage ongoing swelling
What to expect: Continued significant swelling, bruising, and discomfort. Most patients are
surprised by the intensity of the rehabilitation process at this stage. Progress is measured in
degrees of movement and metres walked rather than in large functional milestones. Pain
during exercises is expected and appropriate — within limits your physiotherapist will guide.
Critical milestone: Full knee extension (0 degrees) should be achieved within the first two
weeks. If it has not been achieved, intensive physiotherapy to restore extension is urgently
required — extension deficit that persists beyond three to four weeks becomes
progressively more difficult to correct.
Weeks 3–6: Progressive Rehabilitation
As pain and swelling begin to reduce, the rehabilitation programme becomes more
demanding. This phase focuses on building the strength and movement quality needed for
functional independence.
Goals: Achieve 90 degrees of knee flexion, wean from walking aids, restore normal gait
pattern, begin stair climbing.
Key physiotherapy interventions:
- Progressive range of motion — working toward and beyond 90 degrees of flexion. Most
daily activities require at least 90 degrees; stair climbing requires approximately 110
degrees; sitting comfortably in a low chair requires 120 degrees - Closed kinetic chain strengthening — mini squats, step-ups, leg press at limited range
Stair training — initially step-to pattern (leading with the non-operated leg going up,
operated leg going down), progressing to reciprocal stair climbing - Stationary cycling — an excellent, low-impact rehabilitation tool that simultaneously
improves range of motion and rebuilds quadriceps strength - Balance and proprioception training — the knee replacement disrupts the
mechanoreceptors in the joint capsule; proprioceptive retraining begins here - Hydrotherapy where available — pool-based rehabilitation reduces loading while
maintaining movement quality
What to expect: Meaningful and visible progress. Most patients achieve independence with
daily activities by the end of this phase and are mobile without walking aids. The knee
remains swollen — this is normal and will continue for months. Fatigue from the
rehabilitation effort is significant.
Weeks 7–12: Functional Rehabilitation
The focus shifts from basic mobility to functional performance — restoring the movement
quality and strength needed for the activities of daily life and beginning to address longer
term goals.
Goals: Achieve 110–120 degrees of knee flexion, restore near-normal walking pattern,
improve strength toward functional targets, begin community mobility.
Key physiotherapy interventions:
- Progressive resistance training — increasing loads in squatting, step-up, and leg press
exercises as quadriceps strength improves - Functional movement patterns — sit-to-stand from various chair heights, car transfers,
getting up from the floor, walking on uneven terrain - Walking distance and pace progression — building endurance for community walking
- Low-impact aerobic exercise — walking, cycling, swimming — to rebuild cardiovascular
fitness and support weight management - Continued range of motion work — maximising flexion toward the functional targets of
120 degrees or beyond
What to expect: Growing confidence and independence. Most patients are driving
(automatic vehicles, non-operated right knee) by eight to twelve weeks if cleared by their
surgeon. The knee continues to feel different from a normal knee — this is expected and
normal. Full recovery from knee replacement is a long process; patients should not expect
to feel “normal” at three months.
Months 3–6: Consolidation and Return to Activity
By three months, most patients have achieved functional independence. The rehabilitation
focus shifts to consolidating strength gains, optimising walking quality, and returning to the
activities and lifestyle goals that motivated the surgery.
Goals: Approach full functional recovery, return to recreational activities, achieve
rehabilitation targets set pre-operatively.
Key physiotherapy interventions:
- Progressive strengthening to achieve limb symmetry — the operated leg should
approach the strength of the non-operated leg - Activity-specific rehabilitation — returning to golf, swimming, walking programmes,
cycling, and other low-impact recreational activities that are appropriate after knee
replacement - Education on appropriate and inappropriate activities — high-impact activities (running,
jumping, contact sports, heavy lifting) are generally discouraged after knee replacement
to protect the implant’s longevity
What to expect: Continued gradual improvement. Most patients are significantly better
than they were pre-operatively by three months, but continue to notice improvements for
twelve months or more. Swelling may persist with increased activity for many months — this
is normal and does not indicate a problem.
Months 6–12: Full Recovery
The final phase of recovery. Most patients achieve their maximum functional outcome
between six and twelve months post-surgery, though some continue to notice
improvements for up to two years.
The 12-month reality: Recovery from total knee replacement is a genuinely long process.
Patients and families should understand that the first year after surgery is a rehabilitation
year — a year in which steady, progressive improvement continues, and in which the
commitment to exercise, weight management, and appropriate activity pays the dividends
the surgery made possible.
What Affects Rehabilitation Outcomes
Commitment to physiotherapy. Patients who attend all recommended sessions and
perform their home exercises diligently achieve superior outcomes to those who engage
sporadically. Rehabilitation is not passive — it requires active effort.
Weight management. Excess body weight increases loading on the knee replacement,
slows rehabilitation progress, and increases complication risk. Weight management during
and after rehabilitation is a clinical priority.
Pre-operative fitness. As noted, patients who were fitter before surgery recover faster.
Pain management. Adequate pain control in the early post-operative period allows fuller
participation in physiotherapy. Patients should communicate their pain levels clearly to both
their surgeon and physiotherapist.
Psychological factors. Anxiety, depression, and catastrophising — common in patients who
have lived with severe pain for years before surgery — impair rehabilitation progress and are
important to address.

The Health & Style Post-Surgical Rehabilitation Service
At Health & Style Medical Centre, we provide comprehensive post-surgical physiotherapy
for total knee replacement patients across Abu Dhabi — from the early hospital discharge
phase through to full recovery. We work in close collaboration with the orthopaedic
surgeons at Abu Dhabi’s leading hospitals to ensure that our rehabilitation programmes are
aligned with surgical technique and implant-specific requirements.
Our goal is to ensure that every knee replacement patient we work with achieves the best
possible outcome from their surgery — and that the investment they made in their operation
is fully realised through expert rehabilitation.
Book your post-surgical physiotherapy assessment at Health & Style Medical Centre,
Abu Dhabi.

